
Cobra Election Form Template, Http Nfpbnga Com Wp Content Uploads 2018 06 Nfp Bnga Webinar Upmc Cobra Advantage Final 2 Pdf
Cobra election form template Indeed recently has been sought by users around us, perhaps one of you personally. People are now accustomed to using the internet in gadgets to see image and video data for inspiration, and according to the title of the post I will talk about about Cobra Election Form Template.
- Employee Cobra Template
- Https Www Amben Com Demos Cobra Cobra Brokeradminmanual Pdf
- 2
- Cobra Continuation Of Coverage Request Template
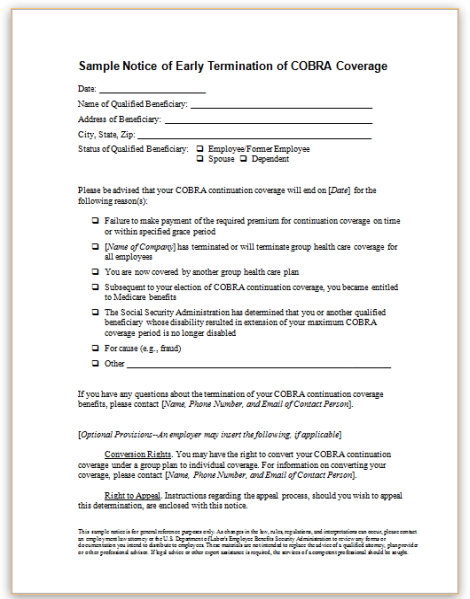
- Cobra Model Election Notice
- Https Www Bcbsnd Com Content Dam Bcbsnd Documents General 65958 4 Bcbsnd Cobra Flyer A6 Lr Pdf
Find, Read, And Discover Cobra Election Form Template, Such Us:
- Group Administration Manual Content Bcbsks
- Human Resources Toolkit Forms American Ambulance Association
- Cobra Open Enrollment Guide 24hourflex
- Employee Cobra Template
- Usa Setting Up Cobra
If you are searching for Presidential Candidates For 2020 Election In Ghana you've arrived at the perfect location. We ve got 104 images about presidential candidates for 2020 election in ghana including images, pictures, photos, backgrounds, and much more. In these web page, we also provide variety of graphics out there. Such as png, jpg, animated gifs, pic art, logo, blackandwhite, transparent, etc.
Cobra Notices And Forms Presidential Candidates For 2020 Election In Ghana

Group Administration Manual Content Bcbsks Presidential Candidates For 2020 Election In Ghana

Salary Change Form Inspirational 9 Salary Change Form Template Estimate Template Change Templates Presidential Candidates For 2020 Election In Ghana
Free 11 Employee Election Forms In Pdf Ms Word Presidential Candidates For 2020 Election In Ghana
Ppt The Cobra Subsidy And The Arra New Information And Trion S Next Steps For Implementation Powerpoint Presentation Id 526053 Presidential Candidates For 2020 Election In Ghana

Bbc News Special Reports 629 629 Election Day How To Vote Guide Presidential Candidates For 2020 Election In Ghana
Start a free trial now to save yourself time and money.
Presidential candidates for 2020 election in ghana. To continue an fsa under cobra the qualified beneficiary must complete and submit th e attached election form to the plan supervisor by sixty 60 days from the date of this notice. Federal law requires that most group health plans. The department of labor has developed a model consolidated omnibus budget reconciliation act of 1985 cobra continuation coverage election notice that the plan may use to provide the election notice.
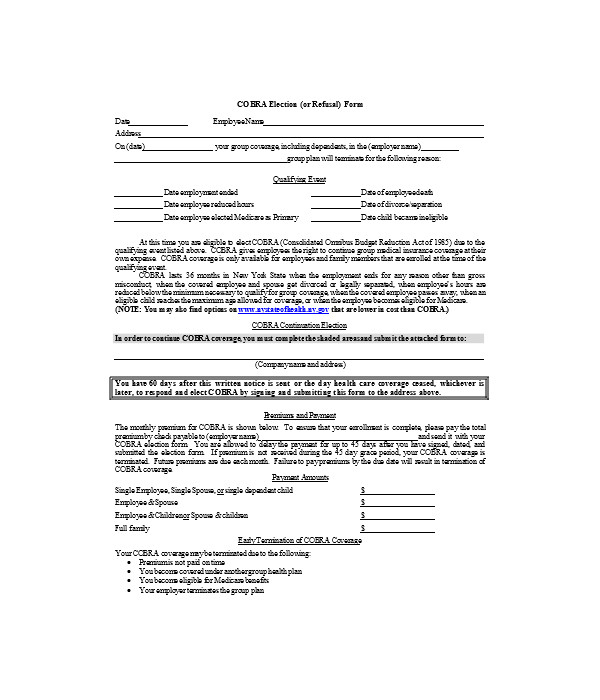
Mail your completed election form to. This election form must be completed in writing and mailed e mailed faxed or hand delivered to companyname. Fill out securely sign print or email your cobra election form 2013 2020 instantly with signnow.
Mail election form check to. This election form should be included in your cobra election packet mkt 171. For faster service you may fax the completed form to 515 376 9043.
To use this model election notice properly the plan administrator must fill in the blanks with the appropriate plan information. The most secure digital platform to get legally binding electronically signed documents in just a few seconds. I do not wish to continue coverage under cobra.
This notice must be sent to the plan participants and beneficiaries by first class mail or hand delivered not later than 14 days after the plan administrator receives notice that a qualifying event occurred. Employers must send notice no later than 44 days after the loss of coverage. Available for pc ios and android.
Cobra administrator station 3w395 po box 9232 des moines ia 50306 9232 if you are submitting a premium payment at this time please attach to the election form. My signature at the bottom of this form represents my stated understanding of all rights and responsibilities as described in the cobra information summary to elect or reject the option to continue coverage through the group fsa plan of the employer. Send completed election form to.
Please retain a copy of the completed election form for your. Epk associates inc. To elect cobra continuation coverage follow the instructions to complete the election form mkt 365 and submit it to the plan administrator at the address below.
15375 se 30th place 380. Please note if you have elected a debit card it will not be reactivated upon cobra election. The completed election form must be postmarked by enter date 60 days from the last date of coverage or from the date of this notice whichever is longer.
Under federal law you must have 60 days after the date of this notice to decide whether you want to elect cobra continuation coverage under the plan. Payment is being sent with the election form please return election form and payment to paymentcompanyname paymentaddress paymentcitystatezip. A valid election of cobra may also be made on our website.
To elect cobra continuation coverage complete this election form and return it to us.
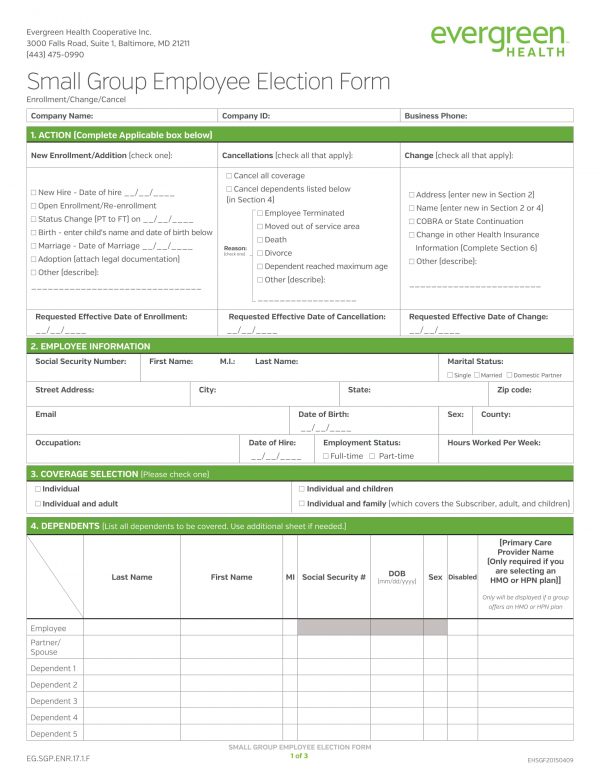
Free 11 Employee Election Forms In Pdf Ms Word Presidential Candidates For 2020 Election In Ghana

New Rule Has Major Cobra Deadline Implications Kistler Tiffany Benefits Presidential Candidates For 2020 Election In Ghana
Cobra Notices And Forms Presidential Candidates For 2020 Election In Ghana
2 Presidential Candidates For 2020 Election In Ghana
More From Presidential Candidates For 2020 Election In Ghana
- Canada Election Map 2015
- Election Card Photo Size
- Presidential Election Laws
- Us Election 2020 News
- Mayor Election 2020
Incoming Search Terms:
- Cobra Qualifying Event Notice Checklist Mayor Election 2020,
- Https Www Mckinneyisd Net Wp Content Uploads 2018 12 Cobra Continuing Coverage For Dental And Or Vision 120518 Pdf Mayor Election 2020,
- Https Pdf4pro Com File 6763 Support Documents 4a Pdf Pdf Mayor Election 2020,
- Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gct 9ecoy968rdbrr0gqcbhv9tqvlpkq7tsw Djrylu3cewoqwa0 Usqp Cau Mayor Election 2020,
- 2 Mayor Election 2020,
- Cobra Elections Cobra Notices Mayor Election 2020,